What is a hernia and what causes it?
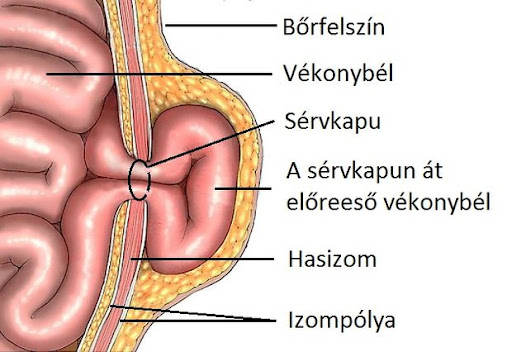
A hernia is defined as the protrusion of an intra-abdominal tissue (intestine, fat, omentum, or part of the peritoneum) from its normal anatomical position through an acquired or congenital opening in the abdominal wall.
The term "hernia" refers to a complex pathophysiology that consists of:
- the hernia orifice (the site where abdominal wall integrity is disrupted)
- the hernia sac – the protruding portion of the peritoneum pushed forward by the hernia contents
- the hernia contents – the abdominal tissue passing through the hernia orifice, which may be fat, omentum, or bowel
What can contribute to hernia development?
Hernia formation can be promoted by any pathological condition that causes increased intra-abdominal pressure:
- Obesity, smoking
- Chronic cough (lung diseases accompanied by chronic coughing)
- Constipation, bowel movement difficulties
- Advanced age (with weakening and loss of elasticity of connective tissues)
- Male sex
Any activity that persistently or significantly increases intra-abdominal pressure may predispose to hernia formation:
- Heavy physical work
- Regular lifting of heavy weights
- Playing wind instruments
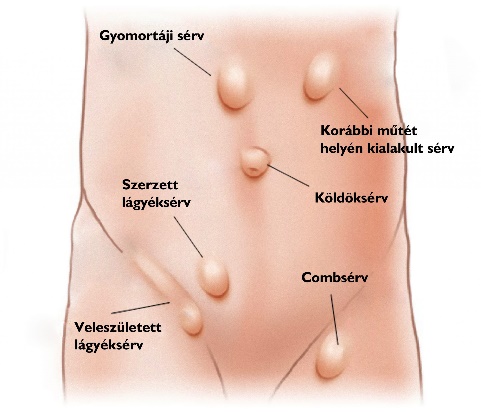
What types of abdominal wall hernias are there?
By location, we distinguish:
1. Groin hernias (inguinal, femoral, obturator)
2. Anterior abdominal wall hernias (umbilical, paraumbilical, epigastric)
3. Atypical or lateral hernias (e.g. Spigelian hernia)
4. Postoperative (incisional) hernias
Hernias developing at the site of a previous surgical incision – approximately 1 in every 10 operated patients is affected! 10% incisional hernia rate!
5. Parastomal hernias
Hernias developing around a stoma (a section of bowel brought out through the abdominal wall)
6. Rectus diastasis
Rectus diastasis (separation of the rectus abdominis muscles) is a condition in which the two straight abdominal muscles running along the front of the abdomen move apart from each other. The connective tissue in the midline of the abdomen stretches and thins, causing the abdominal wall to weaken and the abdomen to "bulge", particularly when straining or sitting up.
What most commonly causes it?
Pregnancy (especially in the case of multiple or twin pregnancies), obesity, smoking, alcohol consumption.
What symptoms can it cause?
Softer, protruding abdomen; a palpable "gap" in the midline of the abdominal wall; lower back pain, postural problems; weakened core muscles.
Important to know:
Rectus diastasis is by definition not a hernia, but if left untreated it can contribute to hernia development and may cause functional problems through changes in abdominal wall anatomy and integrity. Surgical treatment is necessary when it is associated with a developed hernia.
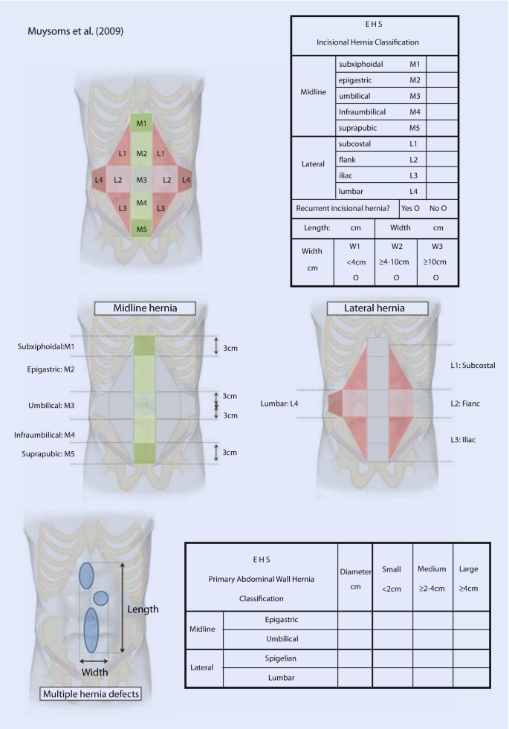
By defect size
| Category | Size | Small | Medium | Large | Giant hernia (loss of domain) |
|---|
By clinical course
- Primary hernia – first presentation
- Recurrent hernia – recurrence after repair
- Multiple recurrences – repeated recurrences
What proportion of the population is affected by hernia-related complaints?
The annual incidence of inguinal hernia alone: approximately 300–350 per 100,000 population in the EU.
Global prevalence – inguinal hernia
According to a worldwide meta-analysis, the prevalence of inguinal hernia is on average 7.7% of the population. Lifetime prevalence of inguinal hernia: men ~27%, women ~3%.
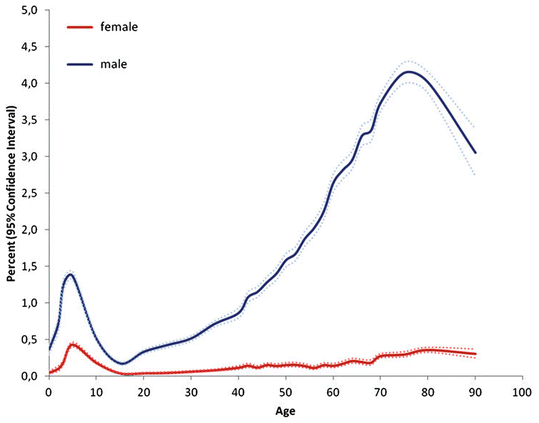
Which age group is affected?
Hernias affect all age groups. The prevalence doubles in those over 45, with the most affected group being those aged 45–75. The highest prevalence is found in those aged 60–75.
How frequently does each type occur?
- ~80% Groin (inguinal and femoral) hernia
- ~10% Incisional hernia
- ~5% Umbilical hernia
- ~4% Paraumbilical hernia
- ~1% Other
A large proportion of acquired abdominal wall hernias are so-called postoperative, incisional hernias. They are caused by inferior scar tissue at the closure line of abdominal surgeries (laparotomies) – affecting 4–10% of operated patients!
Are there hernia types typically associated with a particular sex?
Inguinal hernia is predominantly a male condition. Every man has a 27% lifetime risk of developing an inguinal hernia.
Rectus diastasis: most commonly develops in women following pregnancy, but is also common in obese men.
How wide is the spectrum of possible complaints and consequences?
When should you see a doctor?
Typical symptoms: dull, pressing or pulling pain in the affected area; symptoms typically increase with movement or activity.
A bulge in the skin/abdominal wall or groin area, e.g. after prolonged standing or physical work and sport. The size of hernias increases under exertion.
Important information
Hernias are not in themselves emergency or life-threatening conditions, but they can potentially become life-threatening in the long term and serious complications can develop: hernia incarceration. This occurs when the viscera passing through the hernia orifice become trapped outside the abdominal cavity, compromising the blood supply to the affected bowel loop, leading to bowel obstruction and then bowel necrosis. Emergency surgery is required in the event of incarceration.
What are the alarm symptoms that require immediate action?
- A bulge accompanied by severe pain, possibly with inflamed, reddened skin!
- A known hernia and absence of regular bowel movements, accompanied by abdominal cramps and possibly vomiting!
Risk of incarceration! Seek medical attention immediately, preferably at a surgical emergency department where treatment can be provided on the same day.